What really causes hair loss?
The answer changes everything.
The mainstream explanation — that DHT destroys your hair follicles — is incomplete. A growing body of peer-reviewed research points to a deeper root cause: chronic mechanical tension in the scalp that starves follicles of blood. Understanding this changes how you treat hair loss.
 Updated May 2026
Updated May 2026
 Peer-reviewed evidence
Peer-reviewed evidence
 Comprehensive guide
Comprehensive guide
- The question that broke the DHT theory
- Hair follicles as living mini-organs
- Rethinking DHT's role
- The scalp tension hypothesis
- The cascade: how tension kills follicles
- Clinical proof — the BTX studies
- Six independent lines of evidence
- Common objections answered
- Treatment comparison table
- The practical solution
Why does hair loss always follow the same pattern?
This is the question that cracks the DHT-only theory wide open. If a hormone circulating through your entire bloodstream were the sole cause, why would it consistently destroy hair in one specific, predictable sequence — and leave other hair completely untouched?
The Norwood-Hamilton Scale: a map of something deeper
Male pattern baldness doesn't progress randomly. It follows a precise, well-documented sequence known as the Norwood-Hamilton scale — moving predictably from the temples and crown outward, always in the same order, at the same anatomical locations.
Every man who loses hair follows this same template. Stage 1 → Stage 2 → Stage 3, and so on. The progression is so consistent that researchers built a classification system around it — and it's been validated across cultures, ethnicities, and decades of research.
Here's the problem with the DHT explanation: DHT circulates through your entire bloodstream equally. Your follicles on the sides and back of your head are bathed in exactly the same DHT-containing blood as the follicles on your crown. Yet the crown loses hair. The sides and back do not.

The pattern is the clue. If hair loss were purely hormonal, the pattern would be random — it would vary wildly between individuals. The fact that it follows a rigid, predictable anatomical map means a structural factor is controlling where loss occurs. And that structural factor is scalp tension.
A striking parallel: the man who held his arm up for 30 years
Before we look at the science, consider this illustration. Sadhu Amar Bharati — an Indian holy man — raised his arm as an act of religious devotion and never put it back down. After 30 years, something remarkable happened: his arm withered. Not from disease. Not from infection. Simply from chronically reduced blood flow.
When a limb is held in one position for long enough, the blood supply to its tissues diminishes. Without adequate blood, cells cannot maintain themselves. Tissue atrophies. Structures collapse. Eventually, function is lost entirely.
This is precisely what happens to hair follicles — on a microscopic scale, over years rather than decades, in the specific scalp regions where chronic mechanical forces restrict the blood supply.

What chronic blood flow restriction does to living tissue
Sadhu Amar Bharati's arm demonstrates a fundamental biological principle: living tissue without adequate blood supply cannot sustain itself. The arm received sufficient blood to survive — but not enough for the demanding metabolic work of maintaining muscle mass, nerve function, and structural integrity. The parallel to hair follicles is exact. Follicles are among the most metabolically active structures in the body. They need robust, consistent blood flow to do their job. Without it, they miniaturise and eventually stop functioning altogether.
Hair follicles are living mini-organs
To understand why blood flow matters so much, you first need to understand what a hair follicle actually is — and what it needs to function.
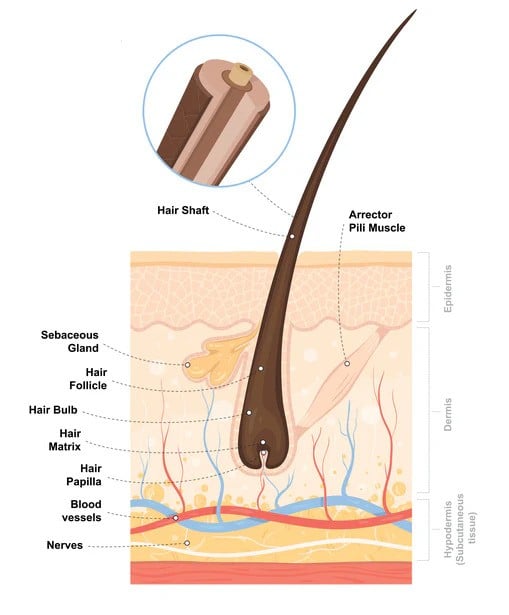
The anatomy of a hair follicle
Each hair follicle is a complex biological structure embedded in the dermis — the middle layer of your skin. At its base sits the dermal papilla (also called the hair bulb): the control centre of the follicle. The dermal papilla is surrounded by a dense network of tiny blood vessels called capillaries.
These capillaries deliver the oxygen and nutrients the follicle needs to produce a hair shaft. The hair growth cycle — anagen (growth), catagen (transition), telogen (rest) — is powered entirely by this blood supply. When the supply is robust, follicles produce thick, healthy hairs and maintain long growth phases. When it's restricted, everything changes.
The follicle begins to produce shorter, finer hairs with each cycle. Growth phases shorten. Eventually, the follicle miniaturises so completely that it produces only a thin vellus (peach-fuzz) hair, then nothing at all. This process — follicle miniaturisation — is the biological mechanism underlying male pattern baldness.
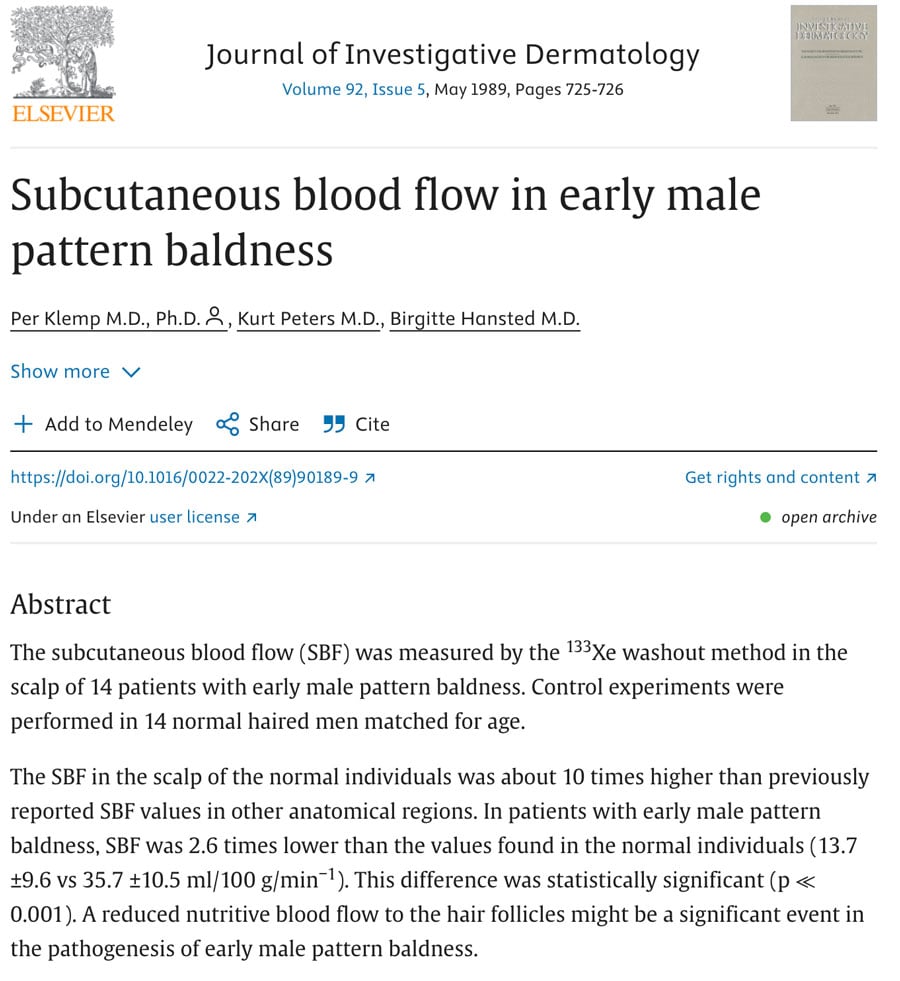
Balding scalps have measurably lower blood perfusion
Multiple independent studies have confirmed that scalp regions undergoing hair loss have significantly lower blood perfusion than hair-bearing regions — even in the same individual. The difference is substantial: some studies measure as much as 2.6× lower blood flow in actively balding zones. This isn't a consequence of the hair being absent — the reduced blood flow is measurable before the hair visibly disappears, and it drives the miniaturisation process itself. Crucially, this blood flow deficit is not distributed evenly across the scalp — it maps precisely onto the pattern of the Norwood-Hamilton scale.
"Hair follicles are the second fastest dividing cells in the human body, after bone marrow. The blood supply demand this places on the dermal vasculature is extraordinary — and any restriction in that supply has immediate and measurable consequences for follicle function."
— Research summary, University of Bradford hair loss studiesDHT is real — but it's not the root cause
DHT absolutely plays a role in male pattern baldness. But the story the mainstream narrative tells is dangerously incomplete — and it matters, because treating a downstream effect while ignoring the root cause is why so many men see limited results from DHT-blocking treatments alone.
What DHT actually does to hair follicles
Dihydrotestosterone (DHT) is a potent androgen hormone derived from testosterone via an enzyme called 5α-reductase. In follicles with certain androgen receptor profiles, DHT binding promotes fibrosis — the formation of scar-like collagen deposits in the dermal papilla and surrounding tissue.
This fibrosis is damaging because scar tissue is much less vascular than normal tissue. It has fewer blood vessels, restricts blood flow, and creates a hostile microenvironment for the follicle bulb. In this sense, DHT directly compounds the blood flow problem.
But here's what the DHT-only theory fails to explain: why does fibrosis happen in some follicles and not others? If DHT were the sole driver, follicles across the entire scalp should be equally susceptible. They're not. And the pattern of susceptibility matches the pattern of scalp tension distribution — not the distribution of DHT or androgen receptors alone.
The eunuch evidence: Hippocrates (c.400 BC) first observed that eunuchs — men castrated before puberty — never go bald. This established that androgens are necessary for AGA. However, when some eunuchs received testosterone supplementation later in life, only those with a genetic predisposition developed baldness. DHT is a necessary input, but something else determines whether and where the follicle damage occurs.
The safe zone problem — DHT's blind spot
The most powerful argument against DHT as the sole cause is what researchers call the "safe zone" — the horseshoe of hair at the sides and back of the scalp that survives even in complete Norwood VII baldness.
Here's what's critical: the hair in the safe zone has DHT receptors. These follicles are exposed to the same systemic DHT as the follicles on the crown. They have androgen-responsive receptor profiles. And yet they remain completely unaffected by AGA.
This is why hair transplants work — donor hair taken from the safe zone retains its "DHT resistance" when moved to the balding crown. But it also reveals the real question: what makes the safe zone safe? The answer is structural. The safe zone has significantly lower chronic scalp tension and consistently better blood flow than the crown and temporal regions. When you fix the blood flow, follicles survive — regardless of DHT levels.
The oxygen-DHT conversion: how blood flow changes your hormone chemistry
Professor B.J. Freund of the University of Arizona identified a remarkable biochemical link between scalp oxygenation and DHT production. The enzyme 5α-reductase — which converts testosterone to DHT — is oxygen-dependent in a specific and critical way.
In low-oxygen environments (as found in compressed, under-perfused scalp tissue), the enzyme preferentially converts testosterone to DHT. In high-oxygen environments (as found in well-perfused scalp tissue), the same testosterone is preferentially converted to estradiol — which actually protects follicles.
This means that scalp tension doesn't just starve follicles of nutrients. By reducing blood flow and therefore oxygen concentration, it actively shifts the local androgen balance toward DHT. The mechanical problem creates the hormonal problem — not the other way around. This is the self-reinforcing cycle that drives progressive hair loss.
"The enzymatic conversion of testosterone to dihydrotestosterone is oxygen-dependent. In low-oxygen environments, the conversion of testosterone to dihydrotestosterone is favoured; whereas in high-oxygen environments, more testosterone is converted to estradiol."
— Professor B.J. Freund, University of ArizonaThe critical reframe: DHT doesn't cause scalp tension — scalp tension causes the conditions (low oxygen, fibrosis) that amplify DHT's damaging effects. DHT is an accelerant poured onto a fire that scalp tension started. This is why DHT blockers help but rarely fully reverse baldness: they address a downstream effect without fixing the structural root cause.
The mechanical root cause of male pattern baldness
The scalp tension hypothesis proposes that chronic mechanical tension in the scalp — created by the muscles surrounding it — is the primary structural driver of androgenetic alopecia. This tension restricts blood flow, promotes fibrosis, and creates the precise conditions in which DHT does maximum damage.
The anatomy of scalp tension: the galea aponeurotica
Your scalp is not simply attached directly to your skull. Between the skin and the bone sits a fibrous sheet called the galea aponeurotica — a tough, inelastic connective tissue structure that spans the top of your head.
The galea connects the frontalis muscle (the large forehead muscle that raises your eyebrows) at the front, to the occipitalis muscle at the back of the skull, and to the temporalis muscles on each side. These muscles are chronically and subtly active — they maintain baseline tension in the galea even when you're completely relaxed.
This creates a permanent, low-level tension across the scalp that pulls the scalp skin taut against the skull. The tension is not uniform — it's highest at the crown (the point furthest from all the anchoring muscles) and lowest at the sides and back (where the muscles insert directly into the scalp). This is not coincidental. It maps exactly onto the Norwood-Hamilton pattern of hair loss.
The galea creates a tent-like structure. Imagine a tent with ropes pegged to the ground around the perimeter. The canvas is most taut — most stretched and compressed — at the centre top. In your scalp, the perimeter muscles are the ropes, the galea is the canvas, and the crown is the apex where tension is highest and blood flow is lowest.

The 3D computational model: a landmark finding
To test the scalp tension hypothesis rigorously, researchers built an advanced 3D finite element model of the scalp — mapping the attachment points of all the scalp muscles and modelling the tension forces they generate. Using this model, they calculated how those forces distribute as compression across the entire dermal surface.
The result was extraordinary. The regions of highest dermal compression in the model corresponded with stunning precision to the regions of earliest and most severe hair loss in the Norwood-Hamilton classification. Stage 2 recession — the temples — matched peak temporal tension zones. Stage 3 vertex — the crown — matched peak superior tension. The "safe zone" at the sides and back showed the lowest computed compression values.
This is not a loose correlation. The match is anatomically precise, stage by stage. No purely hormonal theory predicts this. The tension model does.
This finding cannot be explained by DHT distribution, genetics, or any other systemic factor. It requires a structural, mechanical cause — one that follows the anatomy of the scalp musculature.
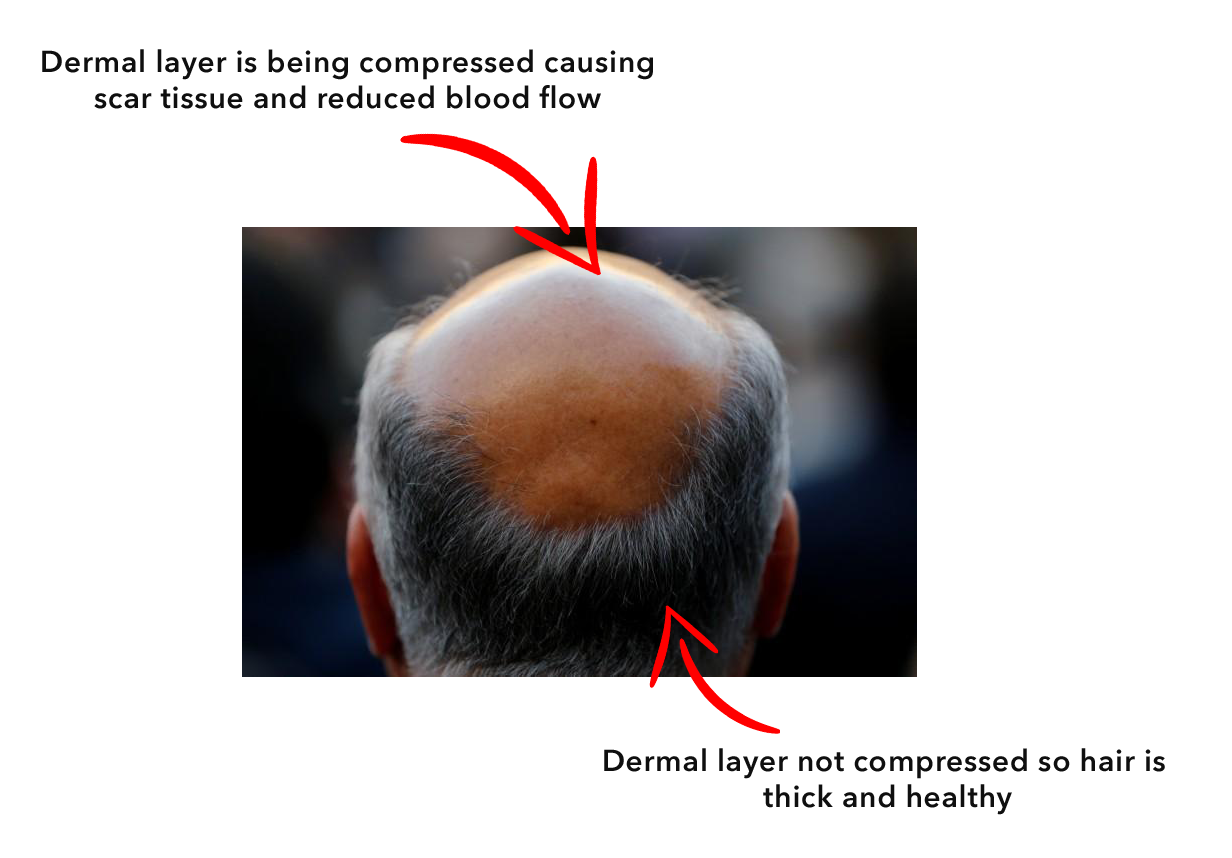

Why the sides and back always survive
In complete (Norwood VII) baldness, a horseshoe of hair at the sides and back of the head remains. This hair persists for life, regardless of DHT levels. From a mechanical perspective, this makes perfect sense: these regions sit directly at the muscular insertion points — where the galea meets the temporalis and occipitalis muscles. The skin here isn't stretched and compressed; it's actually supported by the muscle activity. Blood flow is higher. Fibrosis doesn't develop. Follicles survive. This structural explanation for the safe zone is far more compelling than the alternative — that these follicles are simply "DHT resistant" for unknown reasons.
How scalp tension destroys follicles — step by step
A chain reaction of physical and biological events. Each step makes the next one worse — and this is why hair loss tends to accelerate over time.
Chronic Muscular Tension
The frontalis, temporalis, and occipitalis muscles maintain low-level chronic contraction, creating constant inward and downward tension across the scalp perimeter — mediated through the galea aponeurotica.
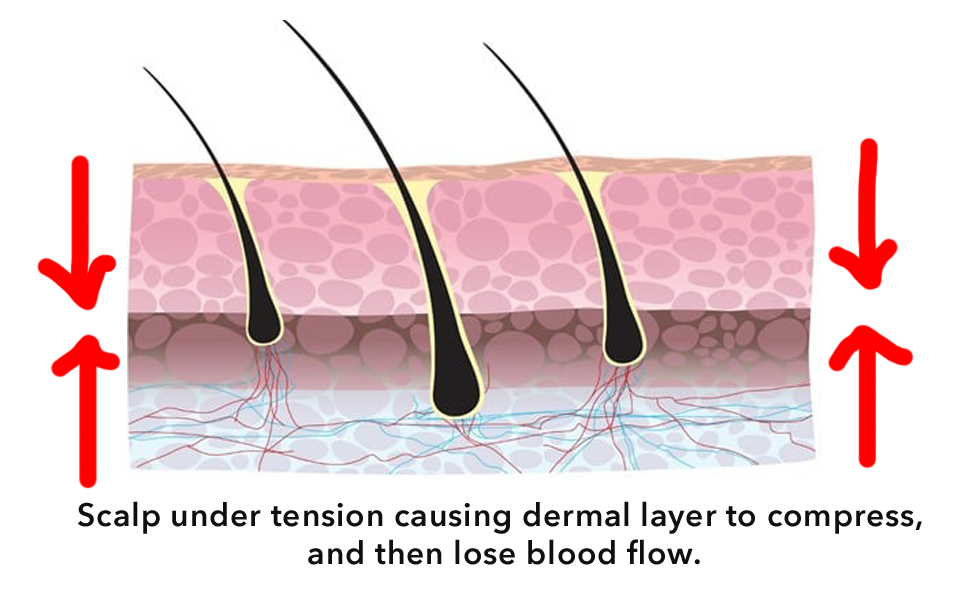
Dermal Layer Compression
The tension compresses the dermis — the thin connective tissue layer where hair follicles live and where the capillaries supplying them run. Compression is highest at the crown and temples.
Blood Vessel Restriction
Compressed dermis narrows the capillaries feeding the follicle bulb. Blood flow — carrying oxygen and nutrients — is measurably reduced. Studies confirm 2.6× lower perfusion in balding zones versus hair-bearing zones.
Oxygen Deficit
Reduced blood flow means reduced oxygen delivery to the follicle. The dermal microenvironment becomes hypoxic — oxygen-depleted. This fundamentally changes local biochemistry, including hormone metabolism.
DHT Amplification
In the low-oxygen environment, 5α-reductase preferentially converts testosterone to DHT rather than estradiol. Local DHT concentration rises — not because of systemic hormone changes, but because of the mechanical conditions scalp tension created.
Fibrosis Forms
Elevated DHT promotes fibrosis — the deposition of dense collagen scar tissue — in the dermal papilla and perifollicular tissue. Scar tissue is even less vascular than normal dermis, further restricting blood flow and creating a self-reinforcing cycle.
Follicle Miniaturisation
Starved of blood, oxygen, and growth factors, the follicle progressively miniaturises with each hair cycle. Each new hair grows back shorter, finer, and weaker than the last.
Follicle Dormancy
Eventually the follicle produces only a translucent vellus hair, then nothing. But crucially: the follicle is usually still present — just dormant. This means reversal is possible if blood flow is restored before permanent damage occurs.
This is why hair loss tends to accelerate. Each stage of the cycle makes the next iteration worse. The only way to break the cycle is to address its starting point: the mechanical tension that initiates the cascade.
"Mechanistically, the scalp behaves like a drum skin with tensioning muscles around the periphery. These muscle groups can create a 'tight' scalp when chronically active."
— Dr. Brian J. Freund, Researcher on scalp tension and androgenetic alopeciaIf tension causes hair loss, relaxing tension should regrow hair
This is how hypotheses become theories. Researchers took the most direct path to proving the scalp tension hypothesis: they injected the scalp-surrounding muscles with a substance that temporarily paralysed them, eliminating the chronic tension — and measured what happened to the hair.
The muscle relaxant studies: isolating tension as the causal factor
Multiple independent research groups conducted clinical studies using botulinum toxin (BTX) injections — the same compound used in cosmetic procedures — injected into the pericranial muscles surrounding the scalp. The injections temporarily blocked muscle contraction, eliminating the chronic downward and inward tension on the scalp for 3–4 months.
This experimental design is elegant because it isolates the variable. No drugs were administered to change hormone levels. No topical treatments were applied to the scalp surface. The only change was the removal of mechanical tension from the scalp-surrounding muscles. If hair regrowth followed, it would be direct evidence that tension — not hormones — was the primary driver.
The results were striking. Across every study conducted, every single participant showed measurable hair regrowth. Some patients showed near-complete recovery in previously thinned areas. The regrowth was clinically significant, clearly visible, and occurred within the treatment window — with no systemic side effects whatsoever.



achieved through the single mechanism of removing scalp muscle tension — no drugs, no topicals
What the BTX studies prove — and what they don't solve
These studies represent the strongest available proof-of-concept for the scalp tension hypothesis. By removing tension — and only tension — researchers produced real, visible hair regrowth. The mechanism is causally established, not merely correlated. However, BTX injections come with significant practical limitations: each treatment costs hundreds to thousands of dollars, must be repeated every 3–4 months as the effect wears off, requires clinical administration, and carries potential risks of spread to nearby muscles. They proved the principle beyond doubt — but they're not a practical long-term solution.
The BTX studies prove causation, not just correlation. In controlled experimental conditions, removing the single variable of scalp muscle tension was sufficient to produce significant hair regrowth. This is the gold standard of scientific evidence — and it definitively establishes scalp tension as a causal factor in androgenetic alopecia, not merely an associated feature.
Six independent lines of evidence — all pointing the same way
The scalp tension hypothesis isn't supported by a single study. Multiple independent lines of research — from different fields, using different methodologies — all converge on the same conclusion.

3D Computational Modelling
Finite element models of scalp tension distribution match the Norwood-Hamilton pattern precisely — stage by stage. No hormonal model predicts this spatial specificity.

BTX Clinical Trials
Injecting scalp muscles with a paralytic agent — with no other intervention — produced 100% regrowth rates across all participants in multiple independent trials.

Blood Flow Studies
Perfusion measurements consistently show 2.6× lower blood flow in balding scalp regions versus hair-bearing regions — even before hair loss is visually apparent.

Scalp Massage Research
A 2019 study of 300 participants found 68% improvement from scalp massage alone — with a clear dose-response relationship. More massage = better outcomes.
PRP Mechanism
Platelet-Rich Plasma therapy works by injecting concentrated blood directly at the follicle site. Its effectiveness is another confirmation that blood supply is the critical variable.

Transplant Biology
Hair transplants fail long-term when underlying tension isn't addressed — the transplanted hairs miniaturise in their new high-tension environment, confirming that location-specific mechanical forces matter more than DHT sensitivity.
Even simple massage works — when done consistently

300 participants. No drugs. Just mechanical pressure.
A 2019 study recruited 300 participants experiencing hair loss and tracked their outcomes with regular self-administered scalp massage — no medication, no topicals, no surgical intervention. 68% of participants saw measurable improvement or stabilisation of their hair loss. The single most predictive variable wasn't technique, timing, or frequency — it was cumulative massage hours. The target: 36 cumulative hours. Participants who achieved this threshold showed the most dramatic results, with some demonstrating near-complete crown recovery. This dose-response relationship is characteristic of a mechanistic effect, not placebo.
Even expensive treatments accidentally prove blood is the answer
PRP — Platelet-Rich Plasma — is a treatment where your own blood is drawn, spun in a centrifuge to concentrate the platelets and growth factors, and then injected directly into the balding scalp. It costs thousands of pounds per session and requires repeat treatments.
It works. And it works for exactly one reason: it massively increases the concentration of blood supply directly at the follicle site. No other mechanism is proposed. The growth factors in PRP are found in normal blood — the reason PRP helps is that it compensates for the chronic blood flow deficit by flooding the follicle with a concentrated blood supply.
Similarly, minoxidil — the most widely used topical treatment — is a vasodilator. It works by widening blood vessels and increasing scalp blood flow. Researchers didn't design it as a hair loss treatment; they noticed hair growth as a side effect when it was being tested as a blood pressure medication. This accidental discovery is one of the most cited pieces of evidence that blood flow is the central mechanism in follicle health.
Why hair transplants fail — and what it proves
The transplant paradox
Hair transplants move follicles from the "safe zone" — the sides and back — to the balding crown. The donor hair carries the DHT-resistant characteristics of its origin site. Initially, the transplanted hair grows well. But without addressing the underlying scalp tension and blood flow deficit, something troubling happens over time.
The transplanted follicles — now embedded in a compressed, under-perfused, fibrotic scalp environment — begin to miniaturise. They're no longer in the low-tension, high-blood-flow zone that kept them healthy. They're now subject to the same mechanical forces that destroyed the original follicles. Without fixing the root cause, transplants become a very expensive temporary fix.
This is precisely what the scalp tension hypothesis predicts. And it's exactly what many patients experience — which is why the most experienced hair transplant surgeons now recommend addressing scalp tension and blood flow alongside any surgical procedure.

Without fixing scalp tension and blood flow, even successfully transplanted hair will eventually thin and miniaturise — making hair transplants an expensive temporary measure rather than a permanent solution.
Answering the critics — the hard questions
The scalp tension hypothesis is compelling — but it raises legitimate questions. Here are the most common objections, and why the evidence addresses them.
If it's about tension, why do women rarely go bald?
This is perhaps the strongest-seeming objection — and it actually supports the hypothesis rather than challenging it. Women experience hair loss very differently from men, and the differences are instructive.
Women's scalps have structurally different mechanical properties. The galea aponeurotica in women is typically less fibrous and more pliable. Women's scalp muscles generate lower chronic tension. Additionally, women have much lower DHT levels — which, as we've established, is the amplifier of the tension-created damage, not the root cause. Without elevated DHT to accelerate fibrosis in the tension-compressed zones, women experience diffuse thinning rather than the patterned progression men see. When women do experience patterned hair loss (as in female-pattern hair loss), it follows the Ludwig scale — which, notably, corresponds to the regions of highest female scalp tension, not a random distribution.
Doesn't genetics cause hair loss? What's the role of DNA?
Genetics absolutely plays a role — but not in the way most people assume. The scalp tension hypothesis doesn't claim genetics is irrelevant. It reframes how genetics contributes.
Your genes determine several factors relevant to AGA: the tone and activity level of your pericranial muscles, the thickness and elasticity of your dermis, the density of androgen receptors in your follicles, and your baseline DHT levels. In other words, genetics determines your susceptibility to scalp tension-driven hair loss — but it doesn't cause the hair loss directly. Tension executes the damage that genetics makes you vulnerable to.
This explains why identical twins can have noticeably different baldness patterns and progression rates, despite sharing identical DNA. Lifestyle factors, stress, sleep quality, and posture — all of which affect scalp muscle tension — influence the actual outcome within the genetic potential.
If DHT blockers (finasteride) work, doesn't that prove DHT is the cause?
Finasteride does work — typically halting progression in about 85% of users, with modest regrowth in some. But this is entirely consistent with the scalp tension hypothesis. In the cascade we described, DHT is a powerful amplifier of the damage caused by tension-induced blood flow restriction. Blocking DHT reduces the amplification — which is why it helps.
But notice what finasteride doesn't do: it doesn't restore scalp blood flow. It doesn't reverse the existing fibrosis. It doesn't change the mechanical tension. This is why most users who stop finasteride lose all gains rapidly — the root cause (tension, restricted blood flow) is still active, and removing the DHT amplifier was the only thing slowing it down. It's treating a symptom effectively, but not addressing the cause.
A more complete protocol addresses both: reduce scalp tension and improve blood flow (the structural root cause) while optionally using DHT blockers to reduce the hormonal amplification of that damage.
What about stress causing hair loss? Doesn't that refute the tension theory?
Actually, stress is one of the strongest supporting pieces of evidence for the scalp tension hypothesis. Here's why.
Psychological stress triggers elevated cortisol — the stress hormone. Cortisol promotes muscle tension throughout the body, including the scalp-surrounding muscles. Chronically stressed individuals have measurably higher pericranial muscle tone. They also tend to adopt forward-head posture and jaw clenching, which increases frontalis and temporalis muscle activation. All of these mechanisms tighten the galea and compress the scalp dermis.
Telogen effluvium — sudden diffuse shedding triggered by acute stress — is a different phenomenon. But chronic stress's contribution to progressive, patterned AGA is very plausibly mediated through exactly the mechanism the hypothesis describes: elevated scalp muscle tension leading to reduced blood flow.
Why do some bald men have thick beards? Doesn't this disprove the DHT theory issues?
This is an excellent observation that's often cited as evidence against DHT's role. Beard follicles are stimulated by DHT — they grow more robustly in response to the same hormone that appears to damage scalp follicles. This paradox is called the "androgen paradox" in dermatology.
The scalp tension hypothesis resolves it elegantly. Beard follicles are not subject to the chronic compressive forces of the galea aponeurotica and pericranial musculature. They're not in a blood-flow-restricted, fibrotic environment. So when DHT acts on them, it does so in a healthy, well-oxygenated microenvironment — and the result is stimulation rather than damage. The difference isn't DHT; it's the structural context in which DHT operates.
What about the eunuch evidence — doesn't that prove DHT causes hair loss?
The eunuch evidence is often misinterpreted. It proves that androgens (including DHT) are necessary for AGA to develop. It does not prove they are sufficient.
When eunuchs castrated before puberty received testosterone supplementation later in life, only those with a genetic predisposition developed AGA — and only in the patterned way described by the Norwood scale. The pattern appeared because the mechanical template — the scalp tension distribution — was already present. The DHT, once introduced, accelerated fibrosis in the already-compressed, already-hypoxic zones. This is exactly what the scalp tension hypothesis predicts: DHT is the accelerant; tension is the fuel source that determines where it burns.
Can you actually reverse hair loss, or is it permanent?
The answer depends on how far along the miniaturisation process has progressed. Hair follicles typically remain present in the scalp long after they stop producing visible hair — they're dormant, not dead. This is why the BTX studies produced regrowth in men who had lost significant hair: the follicles were still there, just starved.
When blood flow is restored — whether through massage, mechanical devices, or tension reduction — dormant follicles can be reactivated. The key window is before the follicle undergoes complete fibrotic encapsulation, which is believed to occur after many years of severe miniaturisation in the most advanced stages. Earlier intervention produces better results. This is why the data consistently shows that addressing the root cause — not just managing DHT — produces lasting improvement rather than temporary symptomatic relief.
How every available treatment measures up
With the root cause established, we can evaluate every hair loss treatment honestly — not by its marketing, but by whether and how it addresses the actual mechanism.
| Treatment | Addresses Root Cause | Improves Blood Flow | Reduces Tension | Side Effects | Results Persist After Stopping | Cost Model |
|---|---|---|---|---|---|---|
| ★ Growband Pro | ✓ Yes | ✓ Sustained | ✓ Cumulative | None | Yes — durable | One-off |
| BTX Scalp Injections | ✓ Yes | ✓ Via tension relief | ✓ Temporary | Minimal local | Partial — fades | Recurring (£££) |
| Manual Scalp Massage | Partial | ✓ Short-term | ✓ Short-term | None | Partial | Free (time-intensive) |
| Minoxidil (Topical) | ✗ No | Temporary only | ✗ No | Mild (shedding, irritation) | No — reverses immediately | Recurring monthly |
| Finasteride (DHT Blocker) | ✗ Partial only | ✗ No | ✗ No | Significant (sexual) | No — reverses on stopping | Recurring monthly |
| PRP Injections | Partial | ✓ Compensatory | ✗ No | Minimal | Partial — requires repeat | Recurring (£££) |
| Hair Transplants | ✗ No | ✗ No | ✗ No | Surgical risks | Fades without root cause fix | One-off (£££££) |
| Laser Caps (LLLT) | ✗ No | Modest improvement | ✗ No | None | Partial | One-off |
| Caffeine Shampoo | ✗ No | Minor surface effect | ✗ No | None | No | Recurring monthly |
Note on combination therapy: The Growband is not in competition with other treatments. Used alongside minoxidil or finasteride, it addresses the root cause while those medications manage downstream effects — producing superior outcomes to any single approach. Many users combine all three for a comprehensive protocol that attacks hair loss from every angle simultaneously.
The practical solution: address the root cause
Scalp massage is proven to work — but accumulating 36 cumulative hours of manual massage is where almost everyone fails. Studies show 95% of people abandon manual routines before reaching the threshold needed for results.
The 36-hour problem
The 2019 scalp massage study identified a clear threshold: participants who accumulated approximately 36 hours of cumulative massage time saw the most dramatic results. Below this threshold, effects were modest. Above it, the improvements were significant and sustained.
The problem is that getting to 36 hours manually is genuinely difficult. Manual massage fatigues your hands and fingers. It's tedious. You lose track of time. You skip sessions. Research confirms that the vast majority of people never get close to the target — not because they don't want results, but because the physical demands of manual massage make consistent adherence almost impossible.
This is the gap the Growband Pro was designed to fill: a hands-free, automated device that accumulates your 36-hour target effortlessly — while you're watching TV, reading, or working.

Scalp Massage
Pushes upward from the perimeter, creating a powerful full-crown massage equivalent — simultaneously across the entire scalp surface.

Tension Reduction
Lifts and grips the perimeter muscles, progressively relaxing chronic pericranial tension with cumulative, lasting effect.
Vasodilation
Pressure-induced vasodilation widens blood vessels and increases scalp perfusion — measurably — during and after each session.


Does it actually increase blood flow?
Researchers attached blood perfusion monitors to subjects and measured scalp blood flow before, during, and after Growband use — in Blood Perfusion Units (BPU).
The data showed a measurable, sustained increase in blood flow to the scalp's dermal layer. Unlike minoxidil — which produces a transient vasodilatory effect lasting perhaps 30–60 minutes — the Growband's mechanical stretching of the pericranial musculature produces a cumulative, progressive relaxation of chronic tension.
With repeated use, this generates lasting improvement in scalp microvascular function — the opposite of pharmaceutical treatments, which reverse completely the moment you stop using them.

Unlike pharmaceutical treatments that require indefinite daily use to maintain any benefit, the Growband's effects are cumulative. Regular use progressively relaxes chronic scalp tension — producing lasting structural changes that don't immediately reverse when you reduce session frequency.


The tissue remodelling advantage
Unlike medications that require permanent daily use to maintain results, consistent mechanical massage creates physical changes to scalp tissue through a process called tissue remodelling. The changes to blood vessel density, dermal elasticity, fibrosis levels, and scalp tension don't vanish the moment you stop treatment.
The BTX studies demonstrated that even temporary removal of scalp tension produces lasting improvements in hair density that persist beyond the treatment period. Mechanical tension reduction through the Growband operates through the same principle — but cumulatively and progressively, building on each session rather than fading between them.
- Fully automated — no hand fatigue or willpower required
- Tracks and accumulates massage time automatically
- Developed by university researchers, not marketers
- Addresses the structural root cause, not just symptoms
- Can be stacked with Minoxidil, finasteride, or caffeine shampoo
- Results improve over time — opposite of drugs that plateau then reverse
- Changes to scalp physiology may persist long after reaching your goal
What Growband users are experiencing
Scalp improvements typically become measurable around 4–8 weeks. Hair density improvements follow within 2–6 months, with results continuing to build over time.



